Add, edit, and delete patient assessments
The initial patient assessment, also referred to as the primary survey, is a critical component of pre-hospital care. This assessment is the basis from which all medical and trauma care decisions are made. You can assess the patient's condition multiple times during treatment, record your findings for each of these assessments.
-
(If you have not done so already) Add a new incident, or open an existing incident, as described Add or edit an incident.
By default, the Scene tab appears.
-
At the bottom of the screen, touch Assessment.
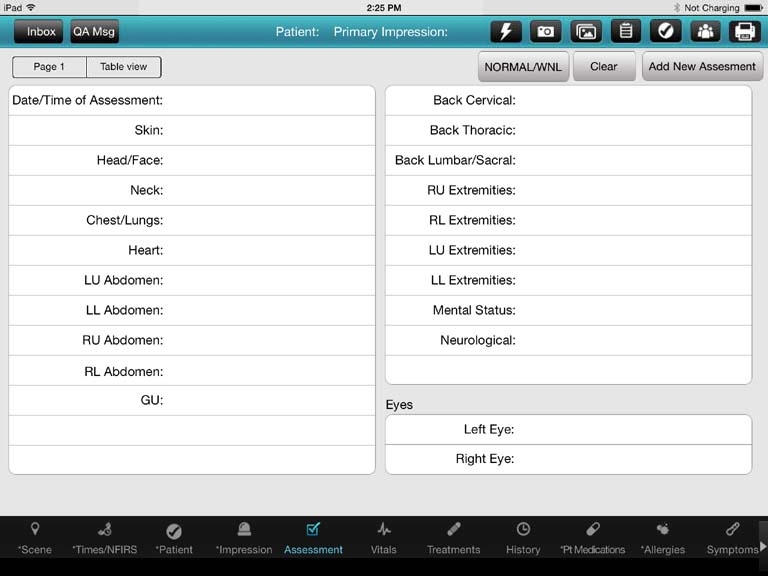
Fields for entering assessment information appear.

-
Do any of the following.
 Add a patient assessment
Add a patient assessment
-
(If you have previously performed an assessment on the patient) Touch Add New Assessment to begin a new assessment with cleared fields.
The data entered in the previous assessment is saved.
-
(Optional, if the results for all or most of the assessments you perform on the patient fall within normal limits for the patient) In the upper left corner of the interface, touch Normal/WNL (within normal limits).
All the assessment fields fill in with a value of
Normal. You can override this value for any individual field with the step below. -
For the fields, enter data (including pertinent negatives) as described in Understand the interface and data entry in it.
Field Information needed Date/Time of Assessment
The date and time the assessment was made.
Skin
A description of the patient's skin appearance, temperature, and moisture level, such as pale, cold, and clammy, or mottled and warm.
Head/Face
Any visible injury to the patient's head, such as a mass, lesion, or swelling, and a description of their initial facial features, such as asymmetric smile or droop. Neck
A description of the patient's neck, such as jugular vein distention (JVD),tracheal deviation, the presence of stoma, and so forth.
Chest/Lungs
A description of the patient's chest and lung function, such as symmetrical rising/falling with each breath, the presence of subcutaneous emphysema (SCE, SE, or Sub Q air), stridor, or crepitus upon palpation.
Heart
Pulse rate, character, rhythm, and other information gathered through auscultation with a stethoscope or other cardiac monitoring systems.
LU Abdomen, LL Abdomen,
RU Abdomen,
RL AbdomenAn assessment of all four quadrants of the abdomen for distension, tenderness, a mass, guarding, entrance and exit wounds, evisceration, painful areas, distention, and discoloration.
GU
A description of the condition and any injuries to the patient's genital and urinary systems (kidneys, ureters, urinary bladder, and urethra).
Back Cervical,
Back Thoracic,
Back Lumbar/SacralPain to range of motion (ROM) in the patient's back, existence of a mass, tenderness in the paraspinal muscles, muscle tightness, and tenderness in the spinous process.
RU Extremities,
RL Extremities,
LU Extremities,
L ExtremitiesA description of any tenderness, swelling, weakness, deformity, contusions, abrasions, burns, bruises, wounds, blood, angulations, abnormal pulses or sensations for the patient.
Mental Status
An assessment of whether the patient is alert and oriented to time, person, place, and date (A+O x 4), or whether they are confused, hallucinatory, combative, or unresponsive.
Neurological
Evaluation of the patient's nervous system, including gait, cranial muscle tone, posture, speech, tremors,or weakness on one side of the body.
Left Eye,
Right EyeAn indication of whether the patient's pupils are equal and reactive to light and accommodation (PERLA), discolored, dialated (and how far), or irregular.
- (Optional) Touch Clear to clear all the entries on the current assessment page.
-
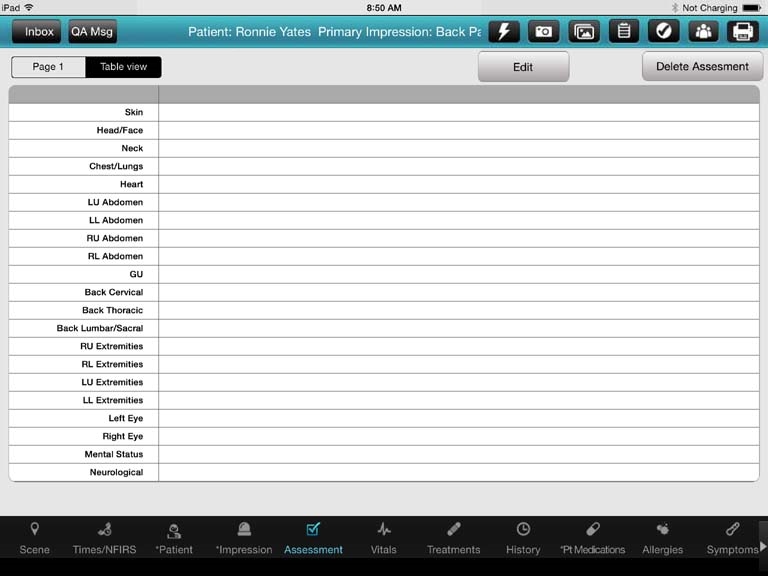
In the upper left corner of the screen, touch Table view.

A summary table listing all the assessments you have performed for the patient appears. This table is useful for comparing assessments side-by-side, and for easily identifying changes between assessments.

Edit a patient assessment
-
In the upper left corner of the screen, touch Table view.
A summary table listing all the assessments you have performed for the patient appears.
-
Touch the heading of the column containing the assessment data you would like to edit.
The entire column highlights.
-
In the upper right corner of the screen, touch Edit.
The Page 1 screen of the assessment appears, populated with the data for that assessment.
- Edit the data as needed.
Delete a patient assessment
-
In the upper left corner of the screen, touch Table view.
A summary table listing all the assessments you have performed for the patient appears.
-
Touch the heading of the column containing the assessment data you would like to delete.
The entire column highlights.
-
In the upper right corner of the screen, touch Delete Assessment.
The assessment is deleted, and its corresponding column in the table disappears.
-